




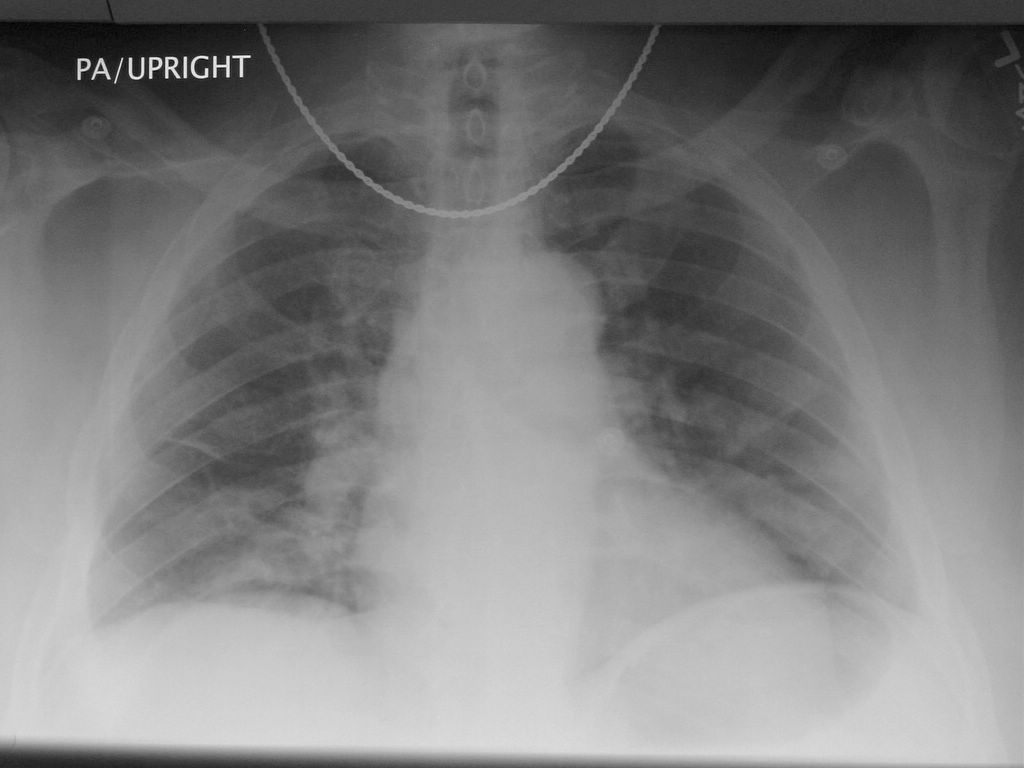
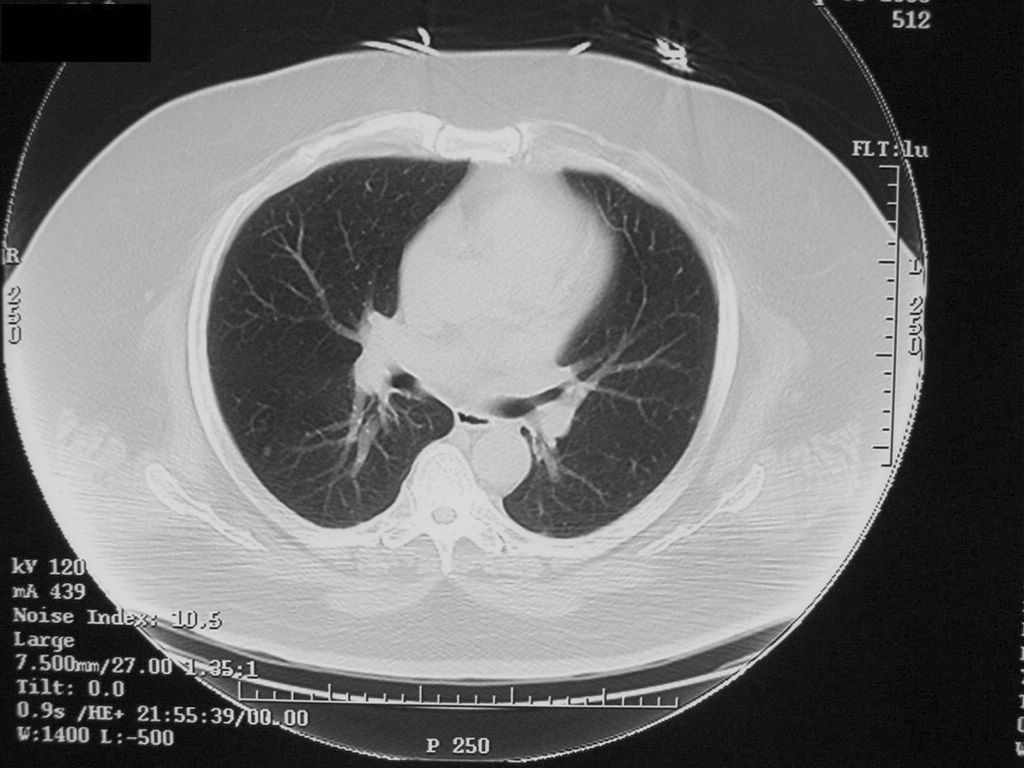
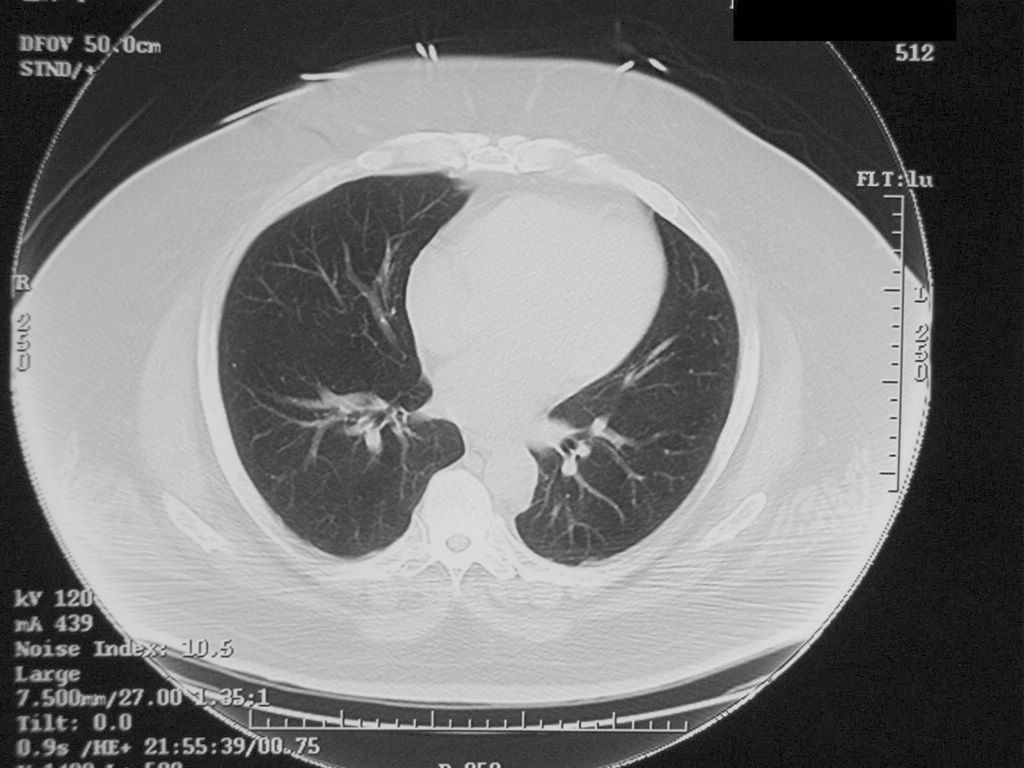
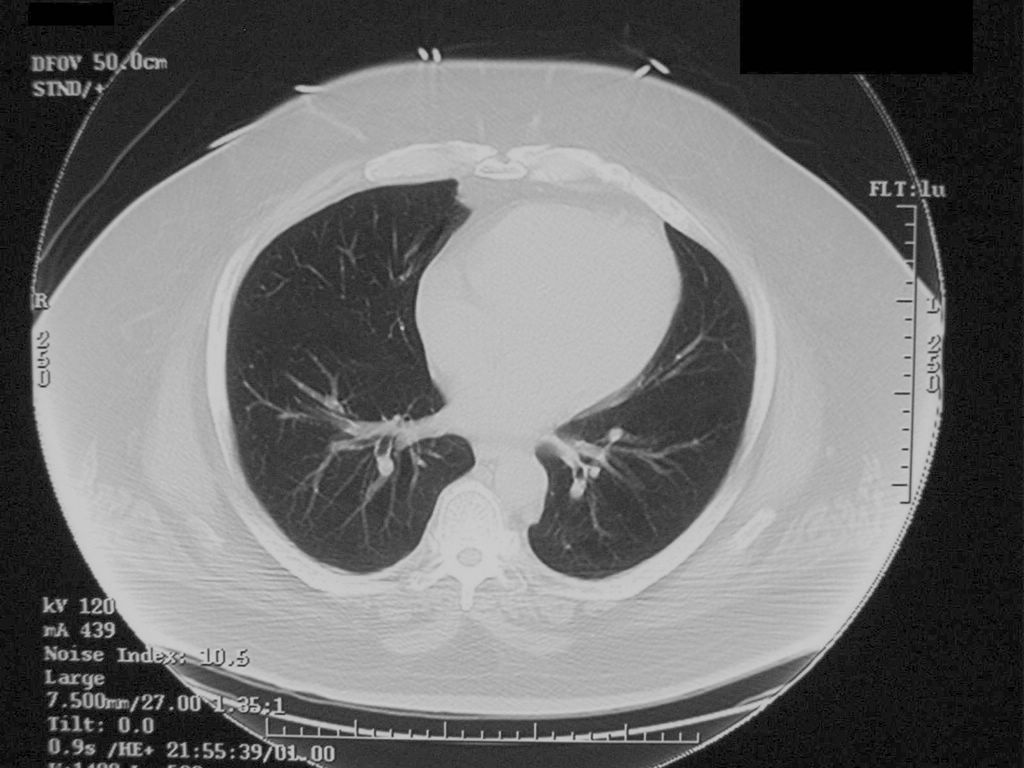
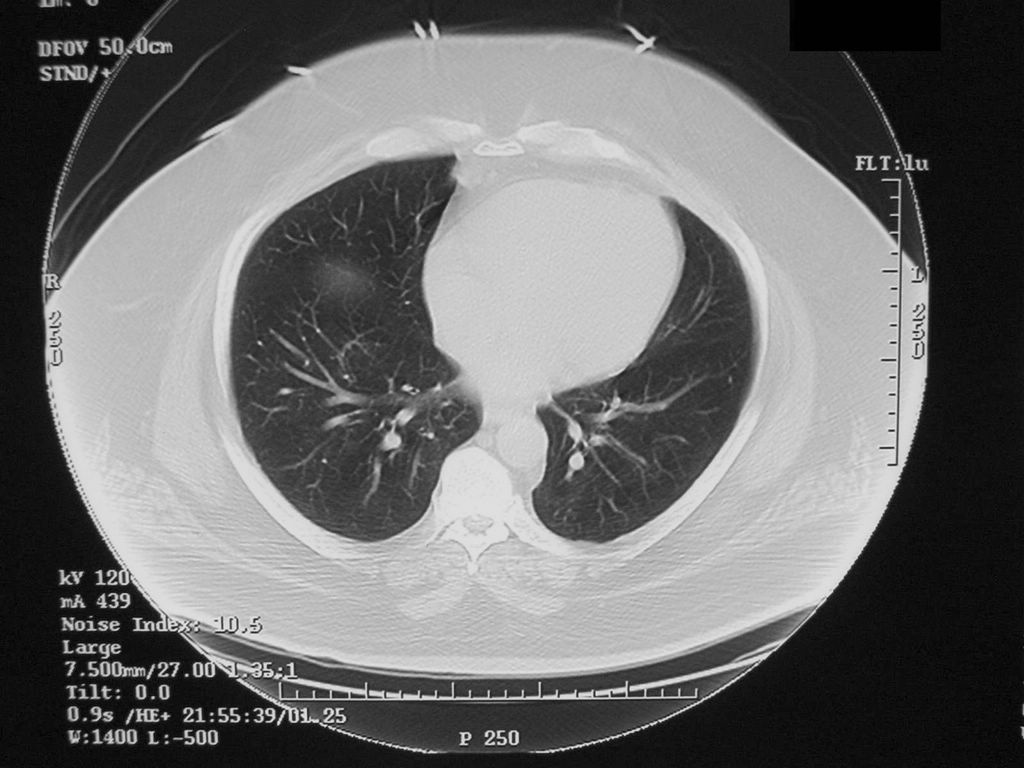
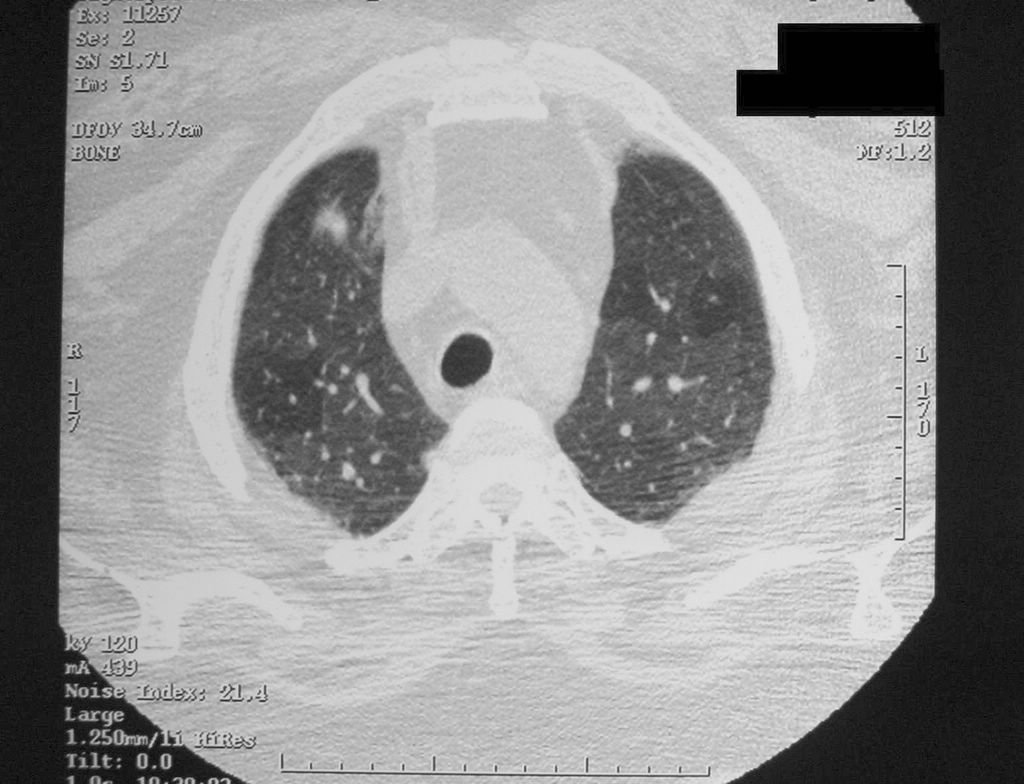
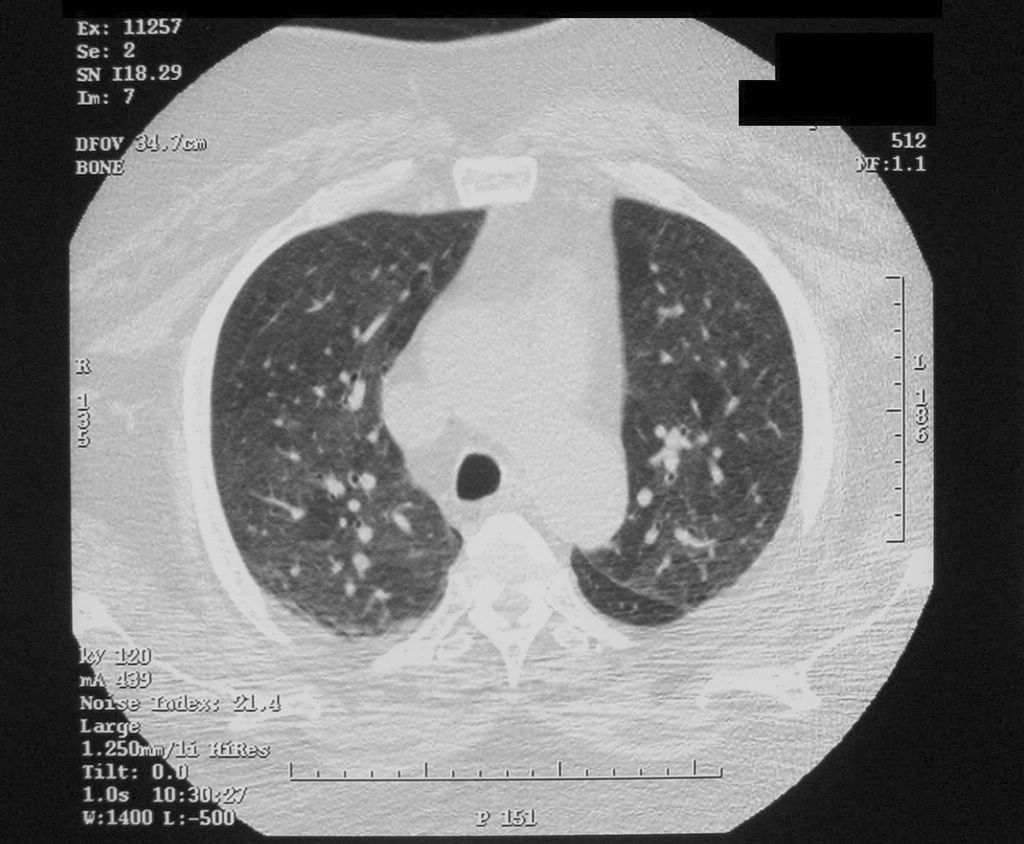
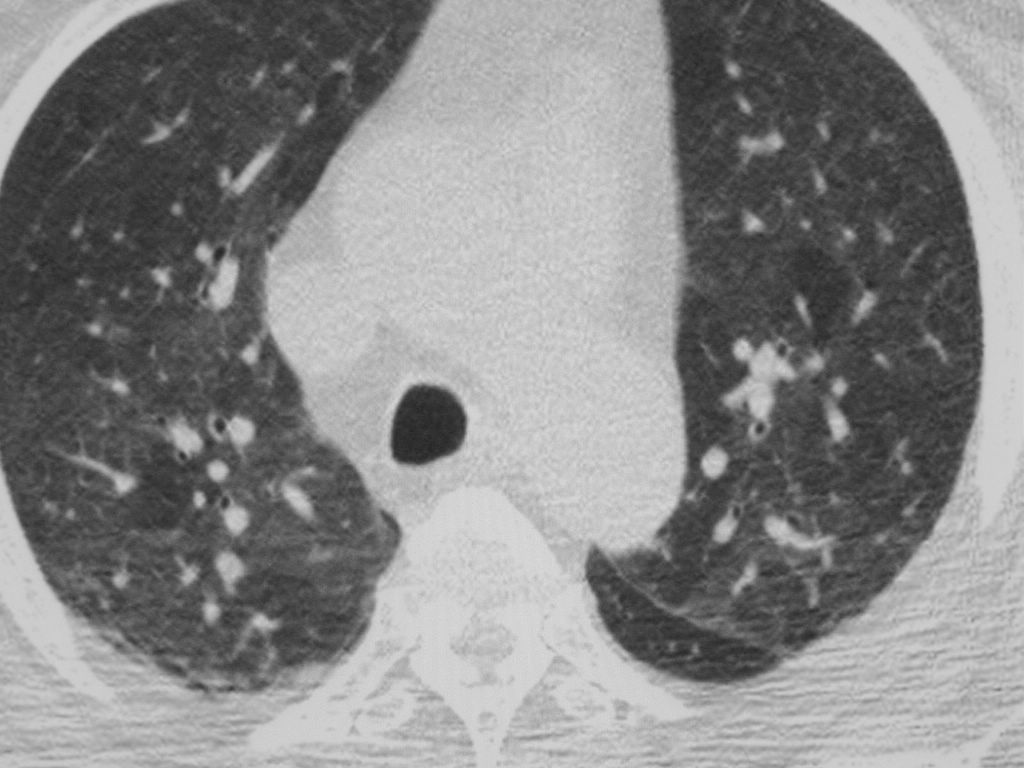
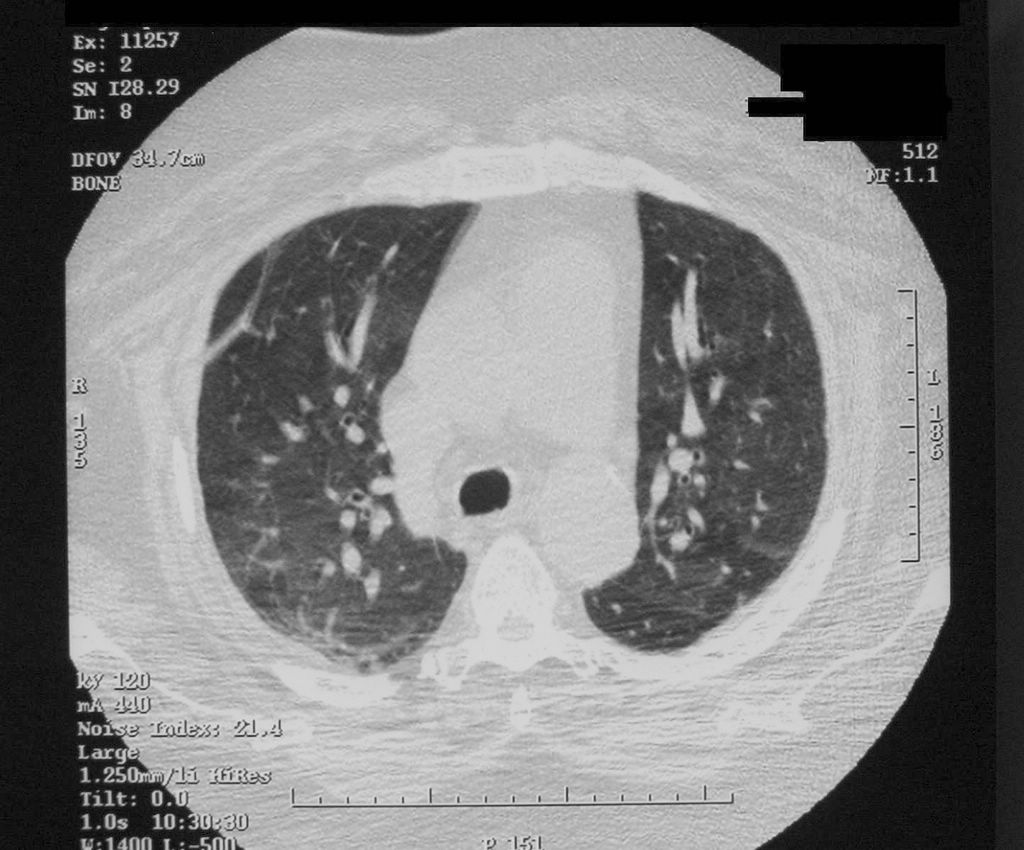
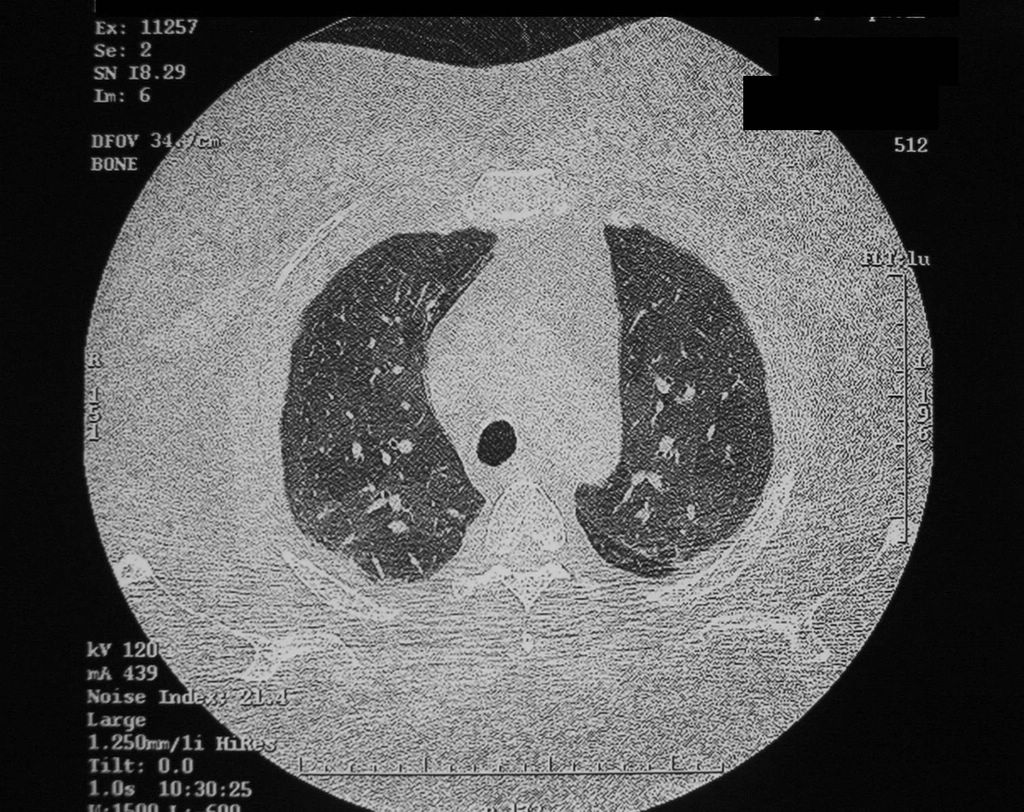
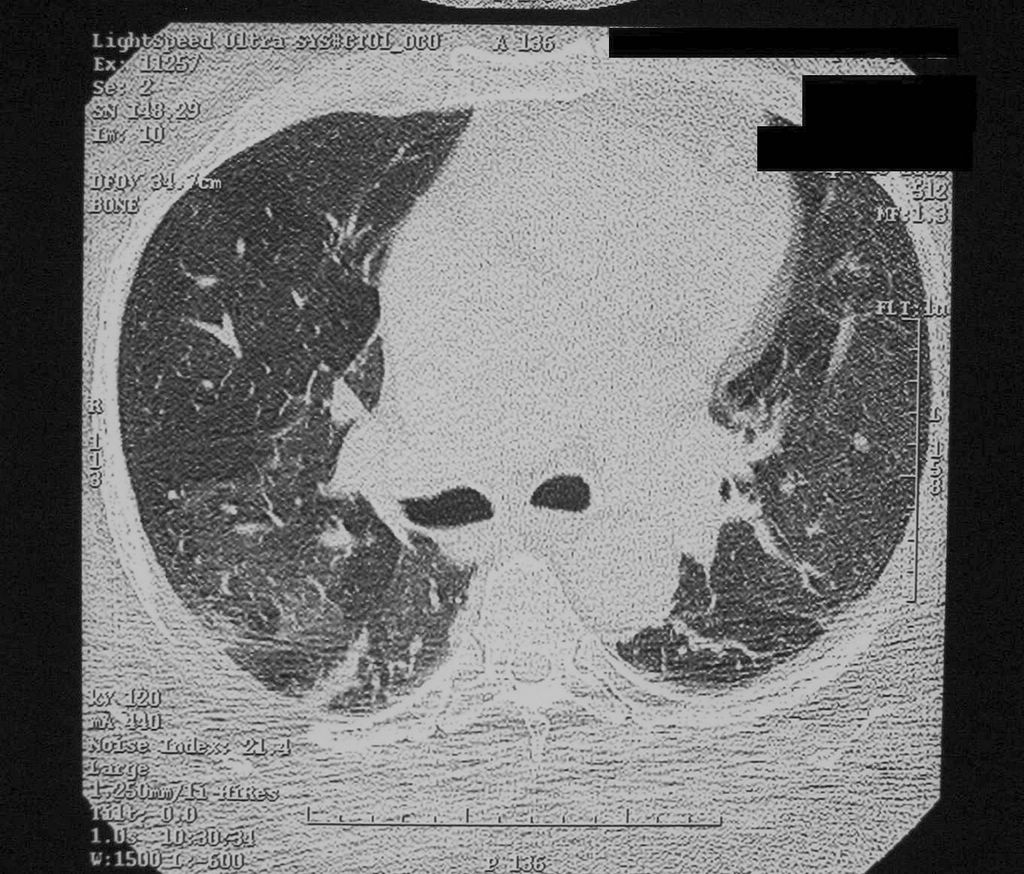
57 yo AAM is admitted to the hospital with SOB for 7 days. He has leg edema which is getting progressively worse, to the point where his scrotum, penis and even his lower abdomen are now edematous. No CP or abdominal pain. He is morbidly obese and has difficulty ambulating, uses a wheelchair at home.PMH: CHF, HTN, DM2, CAD, CRI, BPH, AFib, Gout, OA, OSA on home O2 3 L/min and CPAPMedications: KCl, Coreg, Zocor, Flomax, Lasix, Clonidine, Percocet, Nifedipine XL, Humulin N, aerosols, AmiodaroneFMH: HTNSH: negativePhysical examination:VS 36.4-80-22-160/77SpO2 94% on 3 L/minMorbidly obese, appears mildly tachypneicChest: mild respiratory distress with RR 22, bibasilar ralesCVS: irregularly irregular rhythmAbdomen: obese, soft, generalized anasarca with edema extending up to the level of his umbilicus. His penis and testicles are edematous. He has 2 to 3+ peripheral edema with bilateral Dome wraps on for management of stasis edema.CXR showed pulmonary congestion.CBC, CMPDiagnosis:Right-sided and left-sided CHF.What happened?He was started on Lasix and CPAP.He was ruled out for AMI but he continued to be tachypneic and hypoxic.What happened next?Amiodarone-induced pulmonary toxicity was suspected.The patient was diagnosed with AFib with RVR, difficult to control, approximately one year ago. He was started on Amiodarone 400 mg qd, decreased to 200 mg qd.What are the tests of choice for Amiodarone-induced pulmonary toxicity?High-resolution CT scan of the chestPFTDLCOCT of the chestHigh-resolution CTHigh-resolution CTCT of the chest report:Nonspecific diffuse ground glass mosaic pattern of the lung parenchyma. There are bilateral linear scars or atelectases particularly into the lower lobes and right middle lobe.Impression: Nonspecific ground glass mosaic pattern indicating interstitial lung disease.Follow-up dedicated CT scan of the chest is recommended to confirm.Final diagnosis: Amiodarone-induced pulmonary toxicityWhat did we learn from this case?Amiodarone-induced lung toxicity occurs in 6-15% of the patients treated. A drop of 15% in DLCO helps to make the diagnosis.Toxicity occurs even at the lower Amiodarone doses like 200 mg qd.Treatment is with a corticosteroid trial as with the other idiopathic interstitial lung diseases. There is no RCT proving that steroids are beneficial.References:Prescribing Amiodarone: An Evidence-Based Review of Clinical Indications. JAMA, 2007.Pneumonitis and pulmonary fibrosis associated with amiodarone treatment: a possible complication of a new antiarrhythmic drug. This is the first report of Amiodarone-induced pulmonary toxicity. Circulation.org, 1982.Amiodarone - Reevaluation of an Old Drug. Annals of Int Med.Amiodarone-Induced Pulmonary Toxicity. NEJM Images.Pulmonary Fibrosis, Idiopathic. eMedicine.Amiodarone pulmonary toxicity. VH.org.Amiodarone: Guidelines for Use and Monitoring. AFP 12/2003.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Labels: Cardiology, Pulmonology