




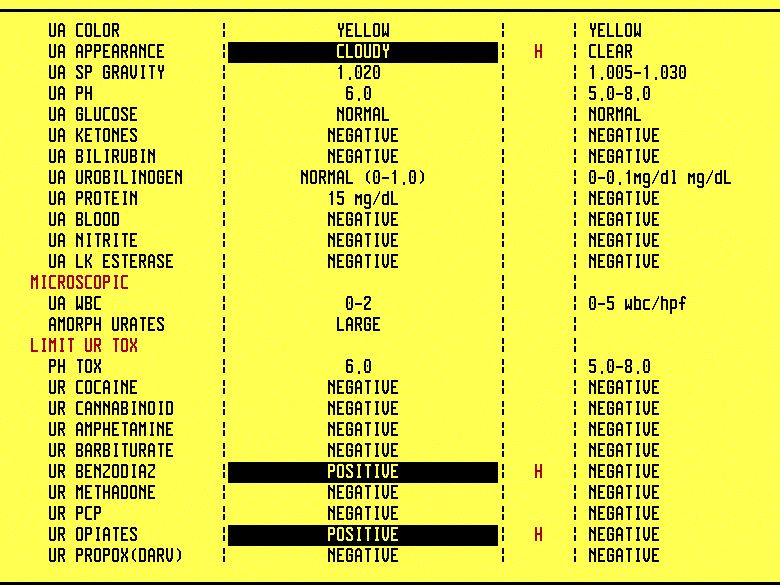
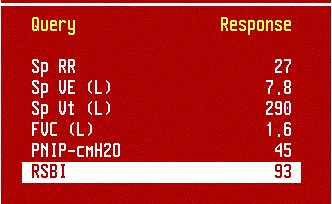
76 yo AAF with COPD was noted to be very lethargic by her family. She takes Vicodin for chronic back pain. On arrival in the ER, the patient is unresponsive. ABG is ordered.PMH: COPD, LBP, DM2, HTNMedications: HCTZ, aerosols, insulin, Vicodin, Ambien, ASAPhysical exam:Obese lady who is visibly SOB and lethargicChest: diminished air entry (B)CVS: Clear S1S2Abdomen: Soft, NT, NDExt: no edemaNeuro: grossly nonfocal, lethargicWhat do you think is going on?Respiratory depression due to opioid and benzodiapine overdose.She was taking Vicodin for chronic back pain and Ambien for sleep.What tests would you order?CBCD, CMPABGCXR, EKGCPP x 2 q 8 hrABG (click to enlarge):ABGs in opioid/BDZ overdose shows respiratory acidosis with compensatory metabolic alkalosis. The patient is a long-term COPD-er and this is the reason for the metabolic compensation. She retains HCO3 to compensate for the the chronic respiratory acidosis.CXR showed COPD changes, EKG was unremarkable.She was intubated because initially she was very lethargic and PaCO2 was 76.Note that first she was on A/C and after a successful CPAP trial, she was extubated.Urine toxic screen shows opiates and benzodiazepinesWhat happened?Narcan is the drug of choice to be given to patients with opioid overdose.She became more awake, the weaning parameters were good (see the picture), and she was successfully extubated.Weaning parameters. The most important one is RSBI (rapid shallow breathing index). If RSBI is less than 100, the chances for successful extubation are more than 85%. Patients who fail the extubation attempt usually develop pulmonary edema or have stridor due to laryngeal edema from the endotracheal tube.After the extubation, she had some wheezing and was treated for a few days with steroids.During the hospital stay, a drop in her nocturnal SpO2 was noted. SpO2 was as low as 82% and dynamic CPAP had to be used.We are virtually certain that she has OSA because she has most of the features - obesity, thick neck, snoring at night, sleepiness during the day, and nocturnal desaturation. She will need a formal sleep study as an outpatient to determine the correct BiPAP or CPAP settings.Final diagnosis: Respiratory failure due to opioid and benzodiazepine overdose.What did we learn from this case?For COPD patients with chronic CO2 retention, it does not take much to push them over the top to acute respiratory acidosis.Be careful when you prescribe opioids in COPD patients. It is better to avoid BDZ. Benadryl can be used as a sleeping aid instead of BDZ.
{kind=link}
{kind=link}
{kind=link}
No comments:
Post a Comment